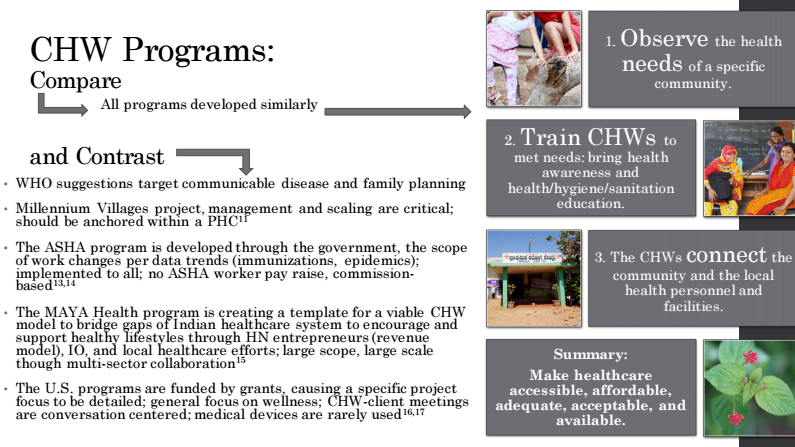
In the last post, I summarized the four community health programs that I've researched this year. Here's a summary of other healthcare points from India and the United States.
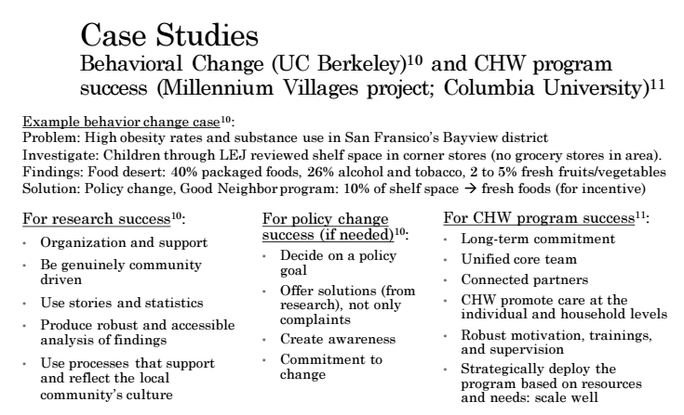
A few case studies influenced the future recommendations that I would have for a community health program like MAYA Health, where I was fortunate to work for the past six months. Here are summaries of the how to implement successful behavioral change and community health worker programs.
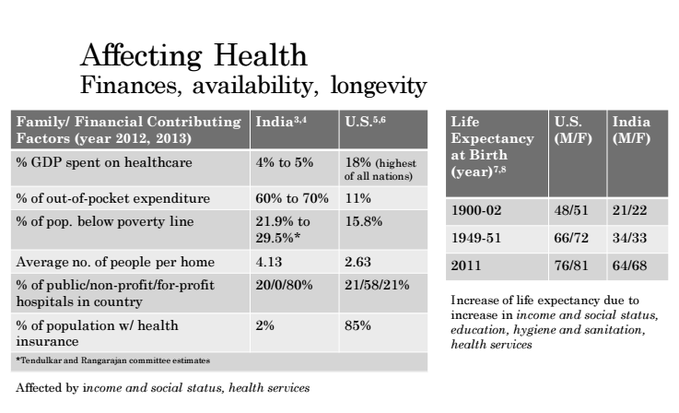
Here are a few factors that should be mentioned when discussing health:
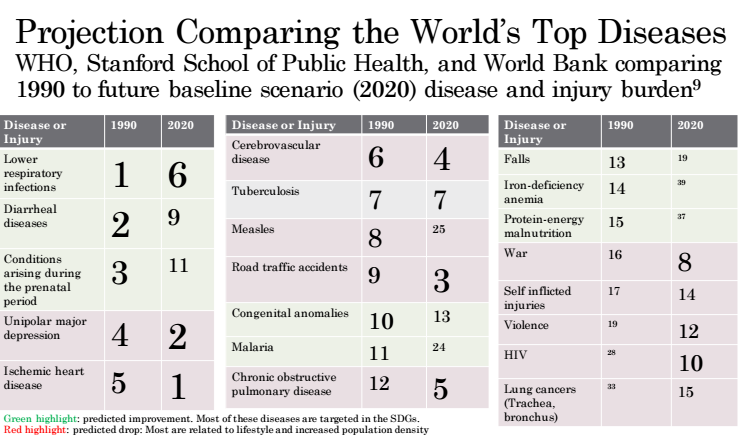
And below is a summary of post- and future projections for the top world diseases from The Global Burden of Disease. It is interesting to see the trend of a decrease in infectious or poverty-based disease like malaria and vitamin deficiency, while there is an increase in non-communicable or 'lifestyle' diseases. It's interesting to think about the decrease of certain illnesses in light of the United Nation and similar program efforts placed on basic food access and eradicating disease. Additionally, the diseases that are increasing (red) are often caused by the increased social and economical pressures of increased work hours, migration, increased intake of quickly accessible foods (that are processed or have excess sugars, salts, and fats), and decreased time in stress-relieving situations (preparing food, exercising, talking with friends).
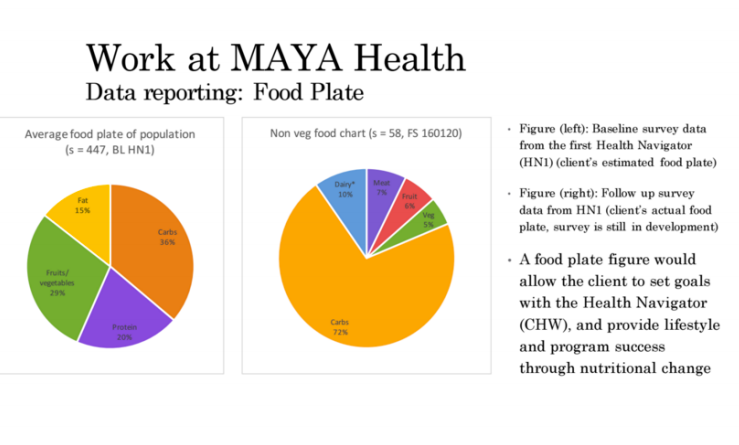
With respect to all of this background knowledge of the current healthcare, I wish to relate it back to community health work and my work at MAYA Health. There are many promising directions for a program like this. Essentially, once a Health Navigator (HN) or a woman appointed by MAYA Health, is trained, she acts as the mediator between a doctor and the community. She builds a relationship with each family, screens patients for illnesses and disease, refers to doctors, and helps to monitor the improvements. I spent this year developing an application through CommCare that would allow the women to do the screening, monitoring, support, and education more easily. By looking at the other community heath programs and also understanding the current and projected needs in healthcare, I was able to more fully develop the application and make recommendations for the program. Below is one example of an image an HN could use to improve client nutrition. Some version of a food plate could be derived from the client's eating habits, and the HN could use it to educate and set goals with the client on nutrition improvements.
Based on research and talking with Bhargavi (mentor) and Dr. Tekur (public health professor and physician), there are a few very practical things that I would recommend to develop health in a community like the one that works with MAYA Health. First, a lot of difficulty comes with affordability and knowledge of food and nutrition. I recommend that a community would buy healthy food in bulk and split the cost. Also, guests could come to host cooking classes and give recipe cards. Finally, a lot of people are disconnected from food. Therefore, I'd recommend that there is a small potted herb and vegetable project where the community grows things like tomatoes and basil, eventually planting it in a community garden.
Other areas that should be addressed include education on water and sanitation: purification, washing, menstrual hygiene, and bathroom use. Often taboos develop around these topics, like women are not supposed to go into temple or in the kitchen, or prepared pickled foods, during their menstruation cycle. Through public health awareness, the community will understand areas of health and eliminate difficult or degrading taboos.
Finally, stress management is difficult. I recommend that there are collective mental health groups within communities that meet to discuss difficulties with alcohol, finance, and other burdens. Also, micro-finance efforts could establish a basic insurance in the community. Finally, basic exercise reduces stress, so walking for a half hour before or after a meal would decrease stress.
(Note to self, these would all be good things to keep in mind for my day-to-day life in the United States, too! :) )
Oofta. Again, I hope that was interesting! It was another semi-long post. If you have any questions about comparisons/contrasts about the Indian and United States healthcare system the details of my work in India, the "take-aways," I would love to discuss them with you! Send me an email/comment. I am no where near an expert, but I have thought a lot about these things, and I enjoy talking about them.
Also, I made this video to briefly capture my time in India. Feel free to take a look!
Thanks for reading.
Other areas that should be addressed include education on water and sanitation: purification, washing, menstrual hygiene, and bathroom use. Often taboos develop around these topics, like women are not supposed to go into temple or in the kitchen, or prepared pickled foods, during their menstruation cycle. Through public health awareness, the community will understand areas of health and eliminate difficult or degrading taboos.
Finally, stress management is difficult. I recommend that there are collective mental health groups within communities that meet to discuss difficulties with alcohol, finance, and other burdens. Also, micro-finance efforts could establish a basic insurance in the community. Finally, basic exercise reduces stress, so walking for a half hour before or after a meal would decrease stress.
(Note to self, these would all be good things to keep in mind for my day-to-day life in the United States, too! :) )
Oofta. Again, I hope that was interesting! It was another semi-long post. If you have any questions about comparisons/contrasts about the Indian and United States healthcare system the details of my work in India, the "take-aways," I would love to discuss them with you! Send me an email/comment. I am no where near an expert, but I have thought a lot about these things, and I enjoy talking about them.
Also, I made this video to briefly capture my time in India. Feel free to take a look!
Thanks for reading.
 RSS Feed
RSS Feed
